Stereotactic Ablative Radiotherapy in AU & NZ
Stereotactic Ablative Radiotherapy (SABR) or Stereotactic Body Radiotherapy (SBRT) both describe an advanced form of radiation therapy that is used to treat many different types of cancer. The two terms are interchangeable.
SABR delivers a very high dose radiation to cancer, which are usually outside the brain.
SABR is painless and no surgery is needed. It is very safe and effective.
People usually get 1-5 treatments.
SABR can be used to cure cancer, such as lung, prostate or kidney cancer.
SABR can also be used to treat cancer that may have spread to different parts of the body, such as bone, lung or liver. This can reduce symptoms and prolong life expectancy in some people. Occasionally, patients treated with this technique may be long-term survivors.
This technique differs from standard external beam radiation therapy as it involves the delivery of higher doses of radiation to the cancer.
SABR uses Xray beams directed from outside the body and using a small number of treatments (also called fractions.
There are several technologies available in Australia that can be used to deliver this technique including Linac based, Cyberknife, Tomotherapy and Gammaknife.
SABR has been made possible by several technological advances. These include the ability to keep patients very still during treatment, tracking the movement of the tumour and more precise and accurate delivery of the radiation therapy.
SABR requires millimetre accuracy. This means special equipment (called immobilisation devices) are usually required to make sure the patient cannot move the body part being targeted during radiation therapy. These include head and neck ‘masks’, vacuum cushions or cradles.
Also, CT scans performed at the time of treatment, using a mini CT built into the treatment machine, ensure accuracy of the treatment delivery.
When the radiation therapy is given to the target (tumour or cancer), the dose is high at this spot but falls off rapidly outside the target. This means there is a low risk of damaging adjacent normal healthy tissues or organs.
In many situations SABR can be an alternative to surgery for small to moderately sized cancers. This avoids the need for an anaesthetic and the risks of an operation, especially for patients who are elderly, frail or have other health issues that might make surgery risky or impossible. At some cancer sites e.g. bone, an operation is not feasible or may be extremely difficult. This is why sometimes SABR is called a ‘minimally invasive’ cancer treatment technique. This special type of radiation therapy is becoming more commonly used and available as the evidence for its use continues to grow.
Specific examples of SABR
Specific examples of SABR include:
Lung SABR: SABR can cure early-stage non-small cell lung cancer and is an exciting new treatment for people with lung cancer who cannot have an operation, or for those who do not want one. Lung SABR may also be a treatment option for patients with secondary tumours from other cancers that have spread to the lung. This may reduce or prevent symptoms and, in some patients, extend life expectancy.
Prostate SABR: Localised prostate cancer can be cured with SABR in carefully selected patients. Evidence from trials shows SABR is emerging as an exciting new alternative to surgery and conventional radiation therapy options with equal cure rates.
Kidney SABR: SABR has also been used in the treatment of primary renal (kidney) cancers in patients that cannot have an operation, or do not want one. SABR can also be used to control secondary deposits in adrenal tumours (located near the kidney).
Bone/Spine SABR: SABR can be used for metastatic disease (secondary cancers) in the bone. The aim is to improve symptoms, such as pain, and quality of life by controlling the cancer in the spine over the longer term. As the spinal cord is often right next to the area being treated, very accurate treatment techniques are used to ensure that this treatment remains safe and effective.
Liver SABR: There is growing use of SABR for the treatment of cancer in the liver. This is for both primary liver cancers such as hepatocellular carcinoma and for secondary cancer (metastases) in the liver. The results from SABR can often be excellent and occasionally, patients treated with this technique may be long-term survivors. By choosing patients who are most suitable for this treatment type, and by sparing of the healthier parts of the liver, serious side effects can be avoided.
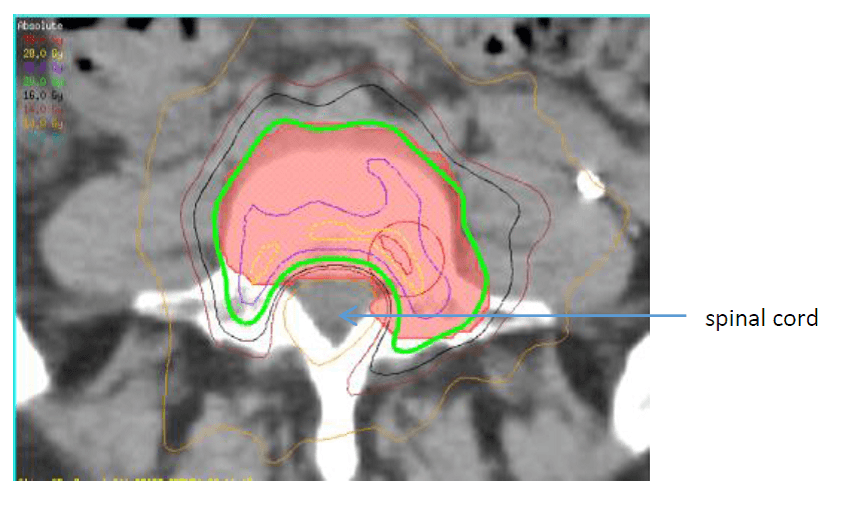
A CT image shows a radiation therapy plan for treatment of a metastasis (secondary cancer) in a vertebra (spine bone). The high radiation dose shown by the green line surrounds the cancerous bone to be treated, shown in shaded red. The spinal cord, which is sensitive to radiation, is spared from getting too much radiation as the high dose is made to wrap around it.
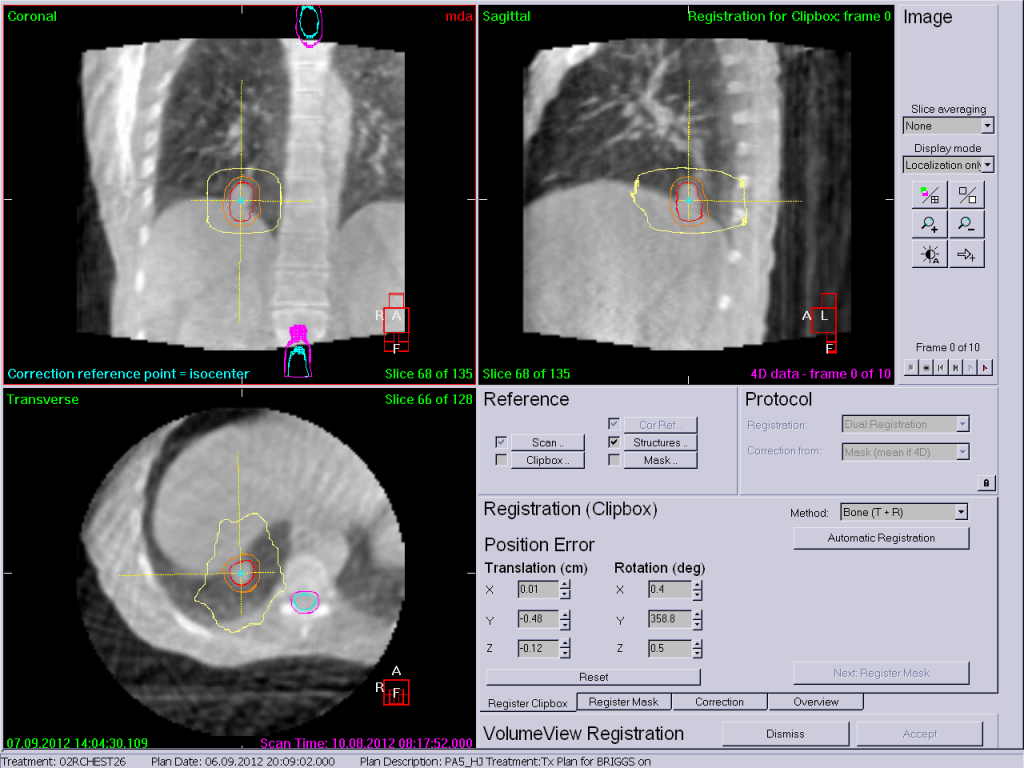
A CT scan taken during radiation treatment is used to ensure the SABR treatment to a lung cancer lines up exactly to the same point every day and remains that way throughout treatment delivery.
Radiation Oncologist
The best person to talk to is a radiation oncologist. You can ask your doctor for a referral to find out if radiation treatment is right for you.
GPs and Health Professionals
Information for any health professional involved in a patient's cancer care with a particular focus on primary care providers.
Talking to Your Doctor
Your GP or other doctors in the cancer team can organise a referral to a radiation oncologist.
Treatment Centres
Search and find your closest Radiation Oncology Treatment Centre.